
Spatial omics makes its debut in pathology
Last century, often termed the “Century of Physics,” Albert Einstein showed that space and time are inextricably entwined. The space-time continuum has been termed the “fabric of our existence.” Today, that continuum is being envisioned in the fabric of our bodily tissues as well as in interstellar galaxies — in the space-time interactions of cells. Cellular arrangements and communication are at the heart of how diseases arise, spread, and how they may be stopped.

All biology happens in space. DNA needs room to replicate. Cells need room to divide. Tissues need room to assemble and fold origami-like. These processes can be visualized. But there are limits. No technology can track the interactions of all 30-plus trillion cells in our bodies. Yet biomedical technologists are not deterred. The emerging field of spatial transcriptomics or spatial omics aims to clarify cellular arrangements and interactions in critical locations of the fabric of life -- our tissues, organs, and structures as Leonardo da Vinci depicted them in his anatomical drawings, which first brought perspective to medical art.
The dawn of spatial omics brings molecular sequencing and imaging together with advances in bioinformatics, giving us the ability to track the spatial activity of biomolecules such as RNA, DNA, and proteins directly in tissue microenvironments, where cancer, inflammation, tissue repair, and drug resistance typically originate. Spatial omics will have a lot to say about how disease is diagnosed in three-dimensional space rather than in two dimensions on microscope slides.
Trac king the changes over time adds a fourth dimension, the temporal. In the near future, pathology will be observed in exquisite detail in a 3D context and in real time. The “flow” of pathobiology – the time travel of disease – begins with a disturbance in the local precincts of what cellular pathology pioneer Rudolf Virchow called the body’s “republic of cells.” Today, we call these spaces tissue microenvironments. In the case of cancer, to know them is to know how we get sick.
king the changes over time adds a fourth dimension, the temporal. In the near future, pathology will be observed in exquisite detail in a 3D context and in real time. The “flow” of pathobiology – the time travel of disease – begins with a disturbance in the local precincts of what cellular pathology pioneer Rudolf Virchow called the body’s “republic of cells.” Today, we call these spaces tissue microenvironments. In the case of cancer, to know them is to know how we get sick.
Three years ago, LMP’s Division of Molecular Pathology and Genomics (MPG) launched a spatial transcriptomics or spatial omics initiative “to study distinct organs and associated disease states” using new laboratory instruments, reagents, and advanced bioinformatics. In 2022, three research projects were funded, all three proposing to illuminate the tumor microenvironment, the space-time continuum of how cancer cells interact with each other and with normal cells in their neighborhood niche and how a malignant tumor originates and grows.
Schwertfeger and Nelson set their sights on breast cancer microenvironments
 LMP professor Kaylee Schwertfeger and associate professor Andrew Nelson and their team are investigating cellular interactions in the breast tumor microenvironment.
LMP professor Kaylee Schwertfeger and associate professor Andrew Nelson and their team are investigating cellular interactions in the breast tumor microenvironment.
Schwertfeger is head of the U of M Masonic Cancer Center's Celluar Mechanisms program. In an LMP Research Forum last year entitled “Tumor heterogeneity and spatial omics in breast cancer,” Schwertfeger focused on macrophages, white blood cells that engulf and kill microorganisms and remove dead cells and how these immune cells in tissue niches are linked to poor outcomes, especially in patients with triple-negative breast cancer (TNBC).
Researchers have identified both tumor-promoting and tumor-suppressing macrophages in breast cancer. Using new technologies and methodologies, Schwertfeger’s team is focused on microanatomic niches where as many as 10 specific macrophage subsets reside interacting with tumor cells in the microenvironment. “We want to identify macrophages with anti-tumor potential because we think those macrophages would signify that those patients might respond well to immune-based therapy because they are poised to do so,” she said in an interview. “We are also interested in identifying subsets of tumor-promoting macrophages. We’re developing new tools that we can use to activate anti-tumor pathways in the pro-tumor macrophages, basically reversing their function so that affected patients may respond to immune therapy whereas normally they wouldn’t.”
Recent studies suggest it may be possible to alter pro-tumor macrophages by activating their latent anti-tumor capability. Schwertfeger is using new antibody approaches to activate anti-tumor pathways by targeting cytokines, immune cell signaling proteins that help the body fight cancer, infections, and inflammation. “We’re generating antibodies that are fused to these cytokines and delivering them specifically to macrophages but not to tumor cells,” she said. The macrophage subtypes on the receiving end of these cytokine-fused antibodies are three of the 10 macrophage subsets: proliferating macrophages, lipid-associated macrophages, and resident macrophages. “Those are the three we focus on in our mouse model. They have very important but distinct functions in the tumor microenvironment.” Could these pro-tumor macrophages subtypes be manipulated to reverse course and, with immune-based therapy, work with other immune cells to eradicate the tumor?
Niches and neighborhoods
Breast cancer can be a heterogeneous tumor with many microenvironments--distinct cellular niches or neighborhoods housing macrophage subsets with a single patient’s cancer. Some niches spur metastases to bone, liver, lung, brain, and other organs.

Spatial technologies, Schwertfeger said, can help identify these niches, define the cellular components and their interactions, and determine how they are regulated. Niches differ in size, number, distribution, and cell populations from patient to patient, but if macrophage behavior can be successfully altered in one or several niches, that may pave the way for successful immunotherapy.
“It’s a hot area,” Schwertfeger said. “Spatial technologies are beginning to be widely used. We’re trying to learn how to use these technologies effectively in mouse models and human breast cancer tissue samples from the I-SPY2 trial.” I-SPY 2 is an adaptive multicenter clinical trial that uses imaging and biomarker analysis to predict a patient’s response to therapy in high-risk breast cancer such as TNBC.
The power of spatial technologies to identify predictive biomarkers in breast tissue specimens was recently illustrated by Schwertfeger-Nelson team member Yuyu He. In a poster presented at USCAP 2024, she focused on breast tumors heterogeneously expressing a progression-associated tumor biomarker called RHAMM (receptor for hyaluronan-mediated motility), which she and her colleagues have earlier shown drives breast cancer invasion. Her experiments revealed patterns of macrophage, T-cell, and B-cell infiltrates in tumor niches with high levels of RHAMM, while spatial gene expression suggested programs of localized immune suppression that may stimulate tumor progression and invasion. He, a laboratory and data scientist in Nelson’s laboratory, used two advanced instruments to generate her data: NanoString GeoMx Human Whole Transcriptome Atlas, which empowers researchers to explore biology across a tissue; and Ionpath’s Multiplexed Ion Beam Imaging (MIBI) in which 20 biomarkers were employed to track immune-cell infiltration at the single-cell level in the tumor microenvironment.
Technology drives the field
This is where the “Century of Physics” comes in. The sophisticated (and expensive) instrumentation needed for spatial omics stems from 20th-century advances in electronics, optics, materials, miniaturization, and, of course, computer technology. The pioneering molecular biologist and Nobel laureate Sydney Brenner famously said that scientific progress depends on new techniques, new discoveries, and new ideas, “probably in that order.” Spatial omics is a case in point. The “omics” refers to the sequencing of DNA (genomics), RNA (RNA-seq), proteins (proteomics), and transcriptomics or the study of the transcriptome—the complete set of RNA transcripts produced by the genome.
Sequencing instruments have made omics possible, and omics has entered clinical medicine in a big way since the completion of the Human Genome Project (HGP) in the early 2000s and the subsequent rise of next-generation sequencing (NGS). Will laboratory instruments illuminate genes and their patterns of expression within tissues in a way that revolutionizes diagnostic pathology, point the way to new therapies, and vindicate proponents of the new science?
Andrew Nelson has taken the lead in introducing laboratory instrumentation to the MPG spatial omics program. In addition to NanoString and MIBI  instruments, he is employing, among others, the Canopy CellScape immunofluorescent spatial imaging and the Visium 10X spatial gene expression platforms. Plus he works with the University’s Spatial omics Services, a partnership between the University Imaging Centers (UIC) and the Genomics Center (UMGC). Because spatial omics is data intensive, Nelson and his colleagues collaborate closely with a team at the Minnesota Supercomputing Institute (MSI).
instruments, he is employing, among others, the Canopy CellScape immunofluorescent spatial imaging and the Visium 10X spatial gene expression platforms. Plus he works with the University’s Spatial omics Services, a partnership between the University Imaging Centers (UIC) and the Genomics Center (UMGC). Because spatial omics is data intensive, Nelson and his colleagues collaborate closely with a team at the Minnesota Supercomputing Institute (MSI).
Besides the breast cancer spatial omics initiative with Schwertfeger, Nelson has been active in the Ovarian Cancer Precision Medicine Initiative (OCPMI) and also SenNet, a research consortium seeking to identify and characterize the differences in senescent cells, cells found throughout the body that have lost their original function and can release substances that may induce or prolong inflammation. SenNet aims to create a senescent cell atlas of spatially mapped senescent cells from imaging and omics data.
Spatial omics instrumentation is in an early stage of development—whether RNA sequencing-based or image-based technologies that read fluorescently-labeled RNA transcripts. Right now, there’s a trade-off. “All these spatial platforms have different levels of resolution,” Nelson said. “The problem is, the fancier the technology, the higher the resolution and the lower the throughput.” Some instruments can only measure small tissue areas at a time-- from 50 to 150 cells, he said. Some are so highly resolved that they can measure gene expression and other activities in either a healthy or diseased single cell. But in the spatial context, the region of interest (ROI) under analysis is key. The throughput -- or how many units of information a system can process in a given amount of time -- is sacrificed with ever-finer resolution.
“When you get really fine resolution, you lose throughput,” Nelson said. “It’s still very much a trade-off. When you do things in a focused way with a set of transcript codes or antibodies, you can make gains in resolution, or you can make gains in throughput. But then when you do things in more unbiased ways, by trying to do unbiased analyses through whole transcriptome sequencing, that’s when you tend to lose either resolution or, more commonly, throughput. And you can only analyze very, very small areas of tissue. That drives how we think about setting up the experiments. We need to know exactly what we’re looking for within the tissue.”
In breast cancer, for spatial omics to have potential prognostic value, square centimeters rather than square millimeters of tissue in an ROI need to be analyzed, and at sufficient resolution. “It’s so heterogeneous, you need to have the capability to analyze fairly large swaths of tissue to begin with in order to find the four or five niches of 500 cells here or there – a niche is less than a square millimeter -- where we say, ‘Hey, this is where we think this biology is going on, this is where this cell-cell interaction is happening, this is the nidus for progression of this disease process,’” Nelson said.
Spatial omics and jellybeans
Nelson reflected on where the field of pathology has been, beginning with the 19th-century cellular pathologist Rudolf Virchow, where it is now, and speculated on where it’s headed. “As pathologists, we were always interested in taking 2D tissue sections and doing careful gross dissections so that we knew where those 2D sections came from -- a 3D organ – and we mapped out all the anatomic structures, all based on histology or low-plex protein stains or cytochemical stains,” Nelson said. “So we knew a lot about anatomy, we knew a lot about tissue histology, we knew a lot about the pathology of it, but the idea of spatial was ‘Can we start understanding the entire transcriptome or much larger swaths of the proteome in the 2D that we usually see on a histology slide?’ That’s what I honestly think is still best labeled as rudimentary spatial technology, where the field of spatial omics is right now.”
To illustrate the challenges that spatial omics pose, Nelson likes to refer to a slide he saw in a talk by OBGYN professor emeritus Timothy Starr. In brief, a jar of jellybeans of all colors is emptied and ground into a fine, homogeneous powder. Then various instruments and methods are applied to identify the specific ingredients. In the case of processed tissue, “We try to measure genes, we try to measure proteins, we try to measure methylation, which affects gene expression. We try to measure all the ‘omics’ things you could do,” Nelson said. “We thought what we really need to do is to analyze gene expression and potentially proteins at the single cell level. So, what are the genes doing in epithelial cells, immune cells, etc? We might learn that there are five different types of epithelial cells based on gene expression. But we don’t know where they are located in the tissue. We don’t know whether they’re around leaky blood vessels. We don’t know if they’re around T cells that can be turned off by tumors. We don’t know if the cells constitute the leading edge of a tumor or if they’re part of the tissue that’s attacking the infectious process, the autoimmune process. We just don’t know where they’re at. At least not yet.”
Schwertfeger and Nelson’s team has a powerful ally in its goal to find out exactly where the cellular action is, -- “where they’re at” -- in breast cancer and spot potential pathways for altered immune cell or drug intervention. As spatial omics instrumentation improves, advanced machine-learning algorithms that can identify tissue networks and patterns by combining single-cell data with megacellular data are in development. “They are absolutely going to become critical,” Nelson said.
In 1959, an IBM scientist coined the term “machine learning” just as the integrated circuit made its debut and two biochemists were awarded the Nobel Prize for their discovery of the mechanisms of DNA and RNA synthesis in cells. Today, the technological battle to defeat cancer by probing its 3D tissue context is joined.
Giubellino and Hamilton Hart set their sights on melanoma microenvironments
In 2011, many patients with metastatic melanoma, a deadly skin cancer, were given a reprieve when the U.S. Food & Drug Administration (FDA) approved a novel immunotherapy called an immune checkpoint inhibitor. In the years since, checkpoint inhibitor drugs have improved remission rates and overall survival for melanoma patients dramatically. But patients tend to relapse.
Melanoma rates have been rising rapidly in the U.S. Despite the more than 70 FDA-approved drugs for treating the disease, many of them immunotherapies, advanced melanoma remains a killer. But if melanoma can be detected and treated while it is still localized, before it reaches the lymph glands, the five-year survival rate is 94 percent, according to the American Academy of Dermatology (AAD). Could melanoma biomarkers be identified in the tumor microenvironment that would inform clinicians which patients would respond to immunotherapy?
 LMP associate professors Alessio Giubellino and Sara Hamilton Hart have set out to answer that question with their MPG spatial omics project “Spatial transcriptomics profiling of melanoma and its immune microenvironment in immunocompromised patients.” Skin cancers including melanoma have a much higher incidence in organ transplant patients undergoing immunosuppressive therapy than the public at large, making these patients good subjects for exploring the details of melanoma cell and immune cell interactions in the tumor microenvironment and identifying predictive biomarkers. Given that immune checkpoint inhibitor drugs produce a lasting remission in a relatively small percentage of patients, “What’s important is to find biomarkers that predict response to therapy,” Giubellino said.
LMP associate professors Alessio Giubellino and Sara Hamilton Hart have set out to answer that question with their MPG spatial omics project “Spatial transcriptomics profiling of melanoma and its immune microenvironment in immunocompromised patients.” Skin cancers including melanoma have a much higher incidence in organ transplant patients undergoing immunosuppressive therapy than the public at large, making these patients good subjects for exploring the details of melanoma cell and immune cell interactions in the tumor microenvironment and identifying predictive biomarkers. Given that immune checkpoint inhibitor drugs produce a lasting remission in a relatively small percentage of patients, “What’s important is to find biomarkers that predict response to therapy,” Giubellino said.
Regions of interest come into focus
Melanoma begins in the epidermis, the skin’s outer layer which contains cells called melanocytes that produce a pigment call melanin. After breaking through the basement membrane, a sheet-like tissue support structure, it invades the dermis and then the subcutaneous tissue region where lymph vessels and blood vessels can transport invasive, metastatic tumor cells throughout the body. Metastatic melanoma typically targets the brain and lungs, though it can invade many other organs. The five-year survival rate for metastatic melanoma is 35 percent.
“We started by analyzing the gene expression profile through RNA analysis in basic melanoma and later in in situ melanoma,” Giubellino said. In situ melanoma is defined by the presence of tumor cells solely in the epidermis, the outer layer of skin. “That’s where melanoma starts. And then we sample early invasive disease [upper dermis], the center of the lesion [mid dermis] and finally the leading edge of the tumor. This leading edge of the tumor is the more advanced portion [spatially] of the disease that will eventually degrade the extracellular matrix [ECM], which serves as a tissue scaffold. After penetrating the ECM it can reach the vessels and metastasize, first to lymph nodes and then systemically to other organs. The size and complexity of the data from our experiments are huge. We are learning how to create guidelines to analyze those data.”
To better understand the interplay between melanoma and immune cells in the tumor microenvironment, Giubellino’s team is employing spatial transcriptomics and proteomics technologies, Nanostring and MIBI platforms among them. Digital pathology powered by deep learning-based algorithms is helping the team to discern morphologic and histopathologic features in formalin-fixed paraffin-embedded tissue sections. By joining omics-derived gene expression profiles with quantitative digital pathology signatures, the team hopes to shed light on the influence of the immune microenvironment on spatial aspects of gene expression in the tumor and guide the development of a minimal panel of genes needed to predict metastatic disease.
Giubellino is focusing much of his team’s effort on the interaction of melanoma cells with immune cells in the tumor microenvironment, including tumor-infiltrating lymphocytes (TILs). He asks: “Can the spatial distributions of TILs and other inflammatory cells be exploited to derive novel biomarkers? Not only the presence or absence of these cells, but also their spatial distribution? Will that affect prognosis or predict immune response to therapy? These are the kind of questions we hope spatial studies will answer.”
Potential answers reside in the spatial gene expression data that’s generated from both sequencing and the Nanostring and MIBI platforms, data that the Minnesota Supercomputing Institute [MSI] bioinformatics team collects and analyzes. “We are interacting with our MSI colleagues to try to get as much spatial information as possible,” Giubellino said. “For us, that means making comparisons across different regions of interest [ROIs] in the tumor following the path of invasion. By comparing, for example, the areas taken from the leading edge of the tumor, we can gauge our ability to see how the invasive portion of the tumor compares in gene expression with the in situ [noninvasive] component in the top layer of skin. This is just an example of how we can add the spatial component to the analysis.”
As we’ve seen, the spatialomics field is driven by instrumentation and massive data. Giubellino hopes the use of additional new spatial and informatics tools, including Lunaphore’s COMET, an end-to-end spatial biology platform, and Nanostring’s AtoMx Spatial Informatics Platform (SIP), a cloud-based platform for spatial biology, “will help us to expand our validation of more tumor-specific biomarkers for melanoma.”
Mice, melanoma, and the immune system
Laboratory mice have been making contributions to melanoma research for a long time. The oncologist Isaiah J. Fidler established protocols for the widely-used B16 melanoma model from mouse cells 50 years ago. In mice, injected B16 cells readily metastasize to lymph nodes and lungs as evidenced by the black melanin pigment they produce, which is easily traced.
Do mice have a role to play in discerning how melanoma cells interact with immune cells in the tumor microenvironment? Hamilton Hart aims to find  out. Hamilton Hart has worked with colleagues in the Center for Immunology to use pet store mice in research. As I wrote in "Hamilton Hart advances the study of immune response with pet store mice" in 2021, she and her colleagues showed that mice from barns and pet stores, so-called dirty mice, recapitulate the human response to pathogens and vaccines more closely than standard laboratory inbred mice, which are genetically homogenous and resemble human newborns just beginning to develop adaptive immunity following exposure to ambient microbes. Since then she has led the Dirty Mouse Colony Core Facility in the Center for Immunology, and she was the opening speaker for a National Institute of Allergy and Infectious Diseases (NIAID) workshop on “Leveraging dirty mice that have microbial exposure to improve preclinical models of human immune status and disease.”
out. Hamilton Hart has worked with colleagues in the Center for Immunology to use pet store mice in research. As I wrote in "Hamilton Hart advances the study of immune response with pet store mice" in 2021, she and her colleagues showed that mice from barns and pet stores, so-called dirty mice, recapitulate the human response to pathogens and vaccines more closely than standard laboratory inbred mice, which are genetically homogenous and resemble human newborns just beginning to develop adaptive immunity following exposure to ambient microbes. Since then she has led the Dirty Mouse Colony Core Facility in the Center for Immunology, and she was the opening speaker for a National Institute of Allergy and Infectious Diseases (NIAID) workshop on “Leveraging dirty mice that have microbial exposure to improve preclinical models of human immune status and disease.”
Because tumor tissue samples under investigation in the melanoma spatialomics project are from immunocompromised patients following their organ transplant, Hamilton Hart is working to recapitulate an immunocompromised status in her models using both normal microbial exposure (NME) mice and standard laboratory mice. Using immunosuppressive drugs in mice that are used in transplant patients proved to be a tricky balancing act. “I had seen in the literature that there were studies using one of these drugs in mice but in patients they are given combination therapy with multiple immunosuppressive drugs at the same time,” Hamilton Hart said. “We wanted to try to model that. Also, in the literature there was little information about what those drugs actually do to immune cells in terms of their reactivity. We didn’t even know if the animals would tolerate the combination therapy that patients receive after their organ transplant. We had to work out dosing schedules and appropriate delivery methods. But the animals were healthy and survived fine.”
After quantifying and characterizing the immune cell populations in the immunosuppressed mice, her team started giving melanoma tumor cells to both drug-treated mice and untreated controls. It took a lot of fine-tuning to find a window of some control of the tumor in the immunocompetent mice but not in the treated [immunosuppressed] mice.” Finding that “window” lays the groundwork for Hamilton Hart to move forward with studies of melanoma cell and immune cell interactions in the murine tumor microenvironment. “We plan to continue to study human samples but also to do more work in the mouse, and using the dirty mice as well, to look at the contribution of different immune cell populations,” Hamilton Hart said. “What will happen if we disrupt macrophages or CD4 T cells that coordinate the immune response? What does that do to the tumor dynamics? We’re measuring things like tumor growth and the activity of tumor-infiltrating cells.”
From the clinical perspective, the team’s goal is to analyze human samples and then move to the mouse to see if a more mechanistic understanding of the disease process in the mouse is possible. Can dirty mice be “leveraged” to improve preclinical models of human immune status and disease? The NIAID workshop concluded that research has demonstrated “that like humans, dirty mice are immune experienced with several examples of improved translational research value in vaccine studies and other immunomodulatory pre-clinical assessments.” Hamilton Hart wonders if the melanoma spatialomics project will provide further evidence that NME mice are a valuable addition to preclinical research. “Another angle from my perspective is, will this be another example of the dirty mice being more relevant than SPF mice [specific pathogen-free standard laboratory mice]?”
Given the clear importance of immune cells like TILs and macrophages in the tumor microenvironment, and given that NME mice have immune systems more closely aligned with humans than SPF mice, NME mice are poised to show us how a tumor tissue niche is a kind of window with a view – a view into how aberrant cells arise and how immune cells govern their spread or their suppression.
Farrar and Tracy set their sights on acute lymphoblastic leukemia microenvironments
No cancer diagnosis strikes fear in the hearts of parents with young children more than acute lymphoblastic leukemia or ALL. The disease accounts for a fourth of all cancers diagnosed in children under the age of 15 in the U.S., with the highest incidence in children ages 1 to 4, according to the American Cancer Society (ACS). Although life extension and cure of ALL through treatment is one of the great biomedicine success stories over the past half century, even successful treatment with current drug regimen carries with it potentially profound long-term side effects. Some 10 to 15 percent of patients relapse following treatment. Most of them become resistant to further therapy, with a high-risk bone marrow or blood stem cell transplant often the last option. Relapsed ALL is the second leading cause of death from cancer in children.
The new immunotherapies have established beyond any doubt that the immune system, with our help, can put ALL at bay and keep it there. The good health of the celebrated Emily Whitehead 12 years after CAR-T cell therapy is evidence of that.
But we need to know more, a lot more about ALL and immunity, about the leukemia’s origin, exceptional complexity, resistance to treatment, and its ability to break free of immune cell constraints and spread from the bone marrow to the spleen, the brain, and other organs.
Spatial omics comes to the blood system
 LMP professor Michael Farrar and his colleague Sean Tracy, assistant professor of medicine, are on the case. Their MPG spatial omics project is entitled “Using spatial transcriptomics and proteomics to track immune responses to leukemia following effective chemotherapies and immunotherapies.”
LMP professor Michael Farrar and his colleague Sean Tracy, assistant professor of medicine, are on the case. Their MPG spatial omics project is entitled “Using spatial transcriptomics and proteomics to track immune responses to leukemia following effective chemotherapies and immunotherapies.”
As Tracy explained in a Masonic Cancer Center talk in 2023, ALL arises when immune cells during lymphopoiesis, the generation of lymphocytes or white blood cells from hematopoietic stem cells (HSCs), become mutated and begin growing rapidly. The two major subtypes are B-cell ALL and T-cell ALL. Clinicians are finding that patients’ initial response to the first rounds of chemotherapy indicate what their long-term outcomes are going to be. Multiple rounds of chemotherapy, especially in pediatric patients, often lead to life-altering long-term toxicities including heart problems, behavior problems, and a variety of secondary cancers.
Relapsed ALL is the second leading cause of death in pediatric cancer. Minimal residual disease (MRD), the presence of a small number of cancer cells in the body following treatment, tends to persist in many patients. Immune cells in the ALL microenvironment – in the bone marrow and lymph system -- are thought to be responsible by inducing an immune suppressive state in that space, paving the way for relapse as the tumor expands. Investigators including Farrar and Tracy are focused on the role of CD4+ helper T cells and other immune cells in the persistence of MRD in treated ALL patients. Leukemia cells exploit various ways to avoid immune recognition and destruction, principally by inducing “tolerance” in these immune cells, which would otherwise clear the tumor. Cancer has a well-earned reputation for co-opting or hijacking the natural immune response to aberrant cells.
“What we think we have right now is a system where what leukemia really does it that it co-ops an existing mechanism to turn T-cells into immunosuppressive cells,” Farrar said in an interview.
“Our hypothesis is that leukemia exists in different states. Those states have different properties. And they exist in different spatial locations.”
Leukemia microenvironments under scrutiny
The chief leukemia microenvironments are the bone marrow, the spleen, and the central nervous system. “For example, the brain is covered by this out layer called the meninges, and that’s where most of the leukemia and the T cells are,” Farrar said. “That’s a very unique environment. We don’t know what ALL is going to look like in the brain versus the bone marrow versus the spleen because all three of those are very different environments. That’s one of the things we’d really like to be able to demonstrate over this next year.”
Preliminary data derived from Farrar and Tracy’s studies, which are funded in part by their MPG spatial omics project, was used in a program project grant (P01) application to the National Institutes of Health (NIH), with Farrar the principal investigator. P01 grants support integrated research projects involving a number of independent investigators who share knowledge and common resources and whose project contributes or is directly related to the common theme of the total research effort. The common theme for three research groups in Farrar’s application is centered around the hypothesis that “ALL-induced immune tolerance plays a major role in initiating relapse and that interventions that prevent or reverse immune tolerance will complement existing front-line treatments by preventing relapse.”
The investigators propose to answer these questions: How does ALL induce immune tolerance? How does combination chemotherapy / immunotherapy prevent relapse? How is immune tolerance induced in different organs? Can ALL specific antigens be identified and used in vaccines to reverse tolerance and prevent relapse? Farrar and Tracy’s team will focus on the mechanisms by which immune tolerance is induced in the bone marrow and spleen. A proposed research core of single-cell and spatial transcriptomics/proteomics technologies will support all three groups.
Immune tolerance is leukemia’s ally
Without a clear understanding of the ways immune tolerance can arise in the leukemia microenvironment in different tissues, experimental treatments are consigned to an empirical “hit or miss” fate, and the chances of failure are high. “Anytime you understand the basic system – how a system works – you can begin to try to think of interventions,” Farrar said. “Until you understand how things work in a nonperturbed system, it’s very hard to come up with effective interventions. You’re left with relatively crude approaches like, well they’re dividing cells, let’s just stop all dividing cells. That is sort of how chemotherapeutics work. They do work but they have massive side-effects.” Farrar contends that if investigators can identify the process of how ALL induces immune tolerance in specific tissue niches – the space where leukemia exerts some control over immune cells – the process potentially can be perturbed or arrested. “That’s an example of how this information could be useful therapeutically,” he said.
Farrar’s foray into spatial omics illustrates well the difficulty of adopting new methods and new technologies, in particular getting complex and costly new laboratory instruments to work as vendors say they should. “They’ve definitely overpromised,” he said. “Most of what has happened since we launched the project has been trying to get the technology to work consistently.” A case in point is the CODEX multiplexed tissue imaging platform, an instrument in the laboratory of LMP hematopathologist Bartosz Grzywac, Farrar’s collaborator on the MPG project who has since left the department. Farrar had to make key ALL antibodies because they were not included in the CODEX instrument’s antibody labeling panel. “We could get CODEX to work, although it took about six months before we were getting usable images. About three months in I was thinking ‘this is never going to work’ but we finally got it to work and we got some data.”
Farrar said he has greater hopes for the Canopy CellScape immunofluorescent spatial imaging platform. “We have, after some fits and starts, gotten a second CellScape instrument to work most of the time. The original instrument was a dud. We got a new version a year ago. That’s when we started to make progress because that instrument actually does work.” Farrar said his laboratory has spent last seven months trying to optimize conditions for how tissue staining is done to use it in CellScape analysis. “Spleen is relatively easy. Bone marrow is harder. But we’ve gotten both of these to work. Doing immunofluorescence on tissues is hard, I’ve discovered. Pathologists who stain tissues regularly can appreciate that.”
Data analysis is yet another challenge. Farrar’s team initially used open-source software. New software can do some “pretty incredible things,” he said, but sometimes format compatibility between instrument exported data and cutting-edge technology like HALO imaging analysis software (“Powering discovery with AI”) is a problem, Farrar said.
“Looking ahead, we’d like to see some nice images of bone marrow, spleen, and also brain where we can track where the leukemia is in these different organs, where the T cells are located that are interacting with the leukemias in them, and how are they interacting with each other,” Farrar said. “That would be a scientific win for us because it would really allow us to look at the cellular level where the different components are interacting in their appropriate neighborhoods.”
And as Farrar insists, without a clear understanding of the ways immune tolerance can arise in the leukemia microenvironment in different tissues, treatments for the leading pediatric cancer will remain less effective and durable than they could be and ALL will continue to exact its toll.
Thyagarajan: Where we are in spatial omics and what’s ahead
 LMP professor and MGP Division Director Bharat Thyagarajan is generally pleased with the progress the three funded spatial omics projects have made, particularly given the technical challenges an emerging scientific field poses and the rapidly evolving commercial instrumentation to which the field is closely tied. As noted in The human genome is poised to reshape clinical medicine published last year featuring Thyagarajan in his capacity as director of LMP’s Advanced Research and Diagnostic Laboratory (ARDL), the clinical application of new scientific fields takes many years, sometimes decades. The National Institutes of Health (NIH) announced the completion of the Human Genome Project in 2003, but it took years before advanced DNA sequencing methods and instrumentation made human genomics practical as a diagnostic tool.
LMP professor and MGP Division Director Bharat Thyagarajan is generally pleased with the progress the three funded spatial omics projects have made, particularly given the technical challenges an emerging scientific field poses and the rapidly evolving commercial instrumentation to which the field is closely tied. As noted in The human genome is poised to reshape clinical medicine published last year featuring Thyagarajan in his capacity as director of LMP’s Advanced Research and Diagnostic Laboratory (ARDL), the clinical application of new scientific fields takes many years, sometimes decades. The National Institutes of Health (NIH) announced the completion of the Human Genome Project in 2003, but it took years before advanced DNA sequencing methods and instrumentation made human genomics practical as a diagnostic tool.
“When I look at spatial omics, it’s very similar to when we started next-generation sequencing [NGS] in 2010,” Thyagarajan said in an interview. “We were barely able to validate the assays before the instrument would be out of date. I would argue that the instrumentation that was needed to do the work didn’t stabilize until 2017 or 2018. I think spatialomics is kind of in the same boat right now.”
Spatial omics may take even longer than genomics to reach the translational science phase and become clinically useful because it’s “more complicated,” Thyagarajan said. The new field combines sequencing with imaging, a powerful partnership but tricky to get right. Typically, there are information “gaps” between what sequencing reveals about a cell’s transcriptome—the cell’s complete pattern of gene expression – and slide-based histological and morphological images. Recently, LMP assistant professor Shijia Zhu and his colleagues published a method in Nature Communications for bridging the gap.
Thyagarajan set two goals for the MPG spatial omics initiative: To establish a best-practices technical platform for the field, and to generate sufficient data for MPG investigators to apply for NIH funding including through program project/center grants (P01).
“When we started the program, I asked the three teams to coordinate in the hope that we would be able to establish best practices for how to do spatialomics,” Thyagarajan said. “What’s the best platform to use? What we’ve found out is that the instrumentation itself is undergoing so many rapid changes that it was not possible to come up with best practices and say, ‘This is the best platform to use.’”
All three groups ended up using their own platform that suited their needs, he said. “From that standpoint, I don’t think the program achieved its goals in terms of what works for research and, from that, providing a platform for translation into the clinic. We are too early in the game in trying to standardize the research findings into one platform.”
The program did succeed in its second goal, Thyagarajan said, by generating spatial omics data to use in applying for NIH funding. One P01 application has been submitted (PI Farrar), another will be submitted soon (PI Schwertfeger), and an R01 application that includes a spatial omics component has also been submitted (PI Giubellino).
The effort to throw light on the space-time nature of cellular pathology in its 3D context will be one of the most data-intensive undertakings in biomedical research. Bioinformatics is a key player. “To make advances in bioinformatics, you first need data,” Thyagarajan said. “Because it’s so new, in our program the investigator who was responsible for generating the lab data was also the person who ended up analyzing the data. So the expertise to collect and analyze the data does exist within our faculty groups now.” The challenge is to generate sufficient spatial omics data using the new tools to meet the program’s goals. “That may take several more years,” he said.
No discussion of data analysis is complete without asking about the potential impact of artificial intelligence (AI) and machine learning on the field. In August, researchers at the University of Pennsylvania published “Unlocking the power of spatial omics with AI” in Nature Methods, noting the potential of multi-modal large language models (LLMs) trained on vast quantities of omics and imaging data to provide an “unprecedented view” into the cellular and molecular organization of disease. “I’m very optimistic about the value of AI in metadata analysis,” Thyagarajan said, consistent with his expressed view of its promise in clinical genomics. “My view is probably overly optimistic. There will be many false steps we take and blind alleys we will go down with AI. But at the end of the day, I like to think of AI as a training tool that is focused on specific questions. That aspect I think will take off, and not just in spatial omics.”
“I actually think one of the most promising applications of AI will be in digital pathology. Then we will take everything we’ve learned in digital pathology and apply it to technologies like spatial omics,” he said.
By integrating spatial omics with histology imaging data, it is possible to imagine that AI can construct high-resolution, comprehensive 3D spatial atlases of tissues, covering an extensive array of omics modalities that reveal the molecular interactions within single cells and within tissue niches. As we have seen, these niches retain some of the space-time secrets that cancer still holds.

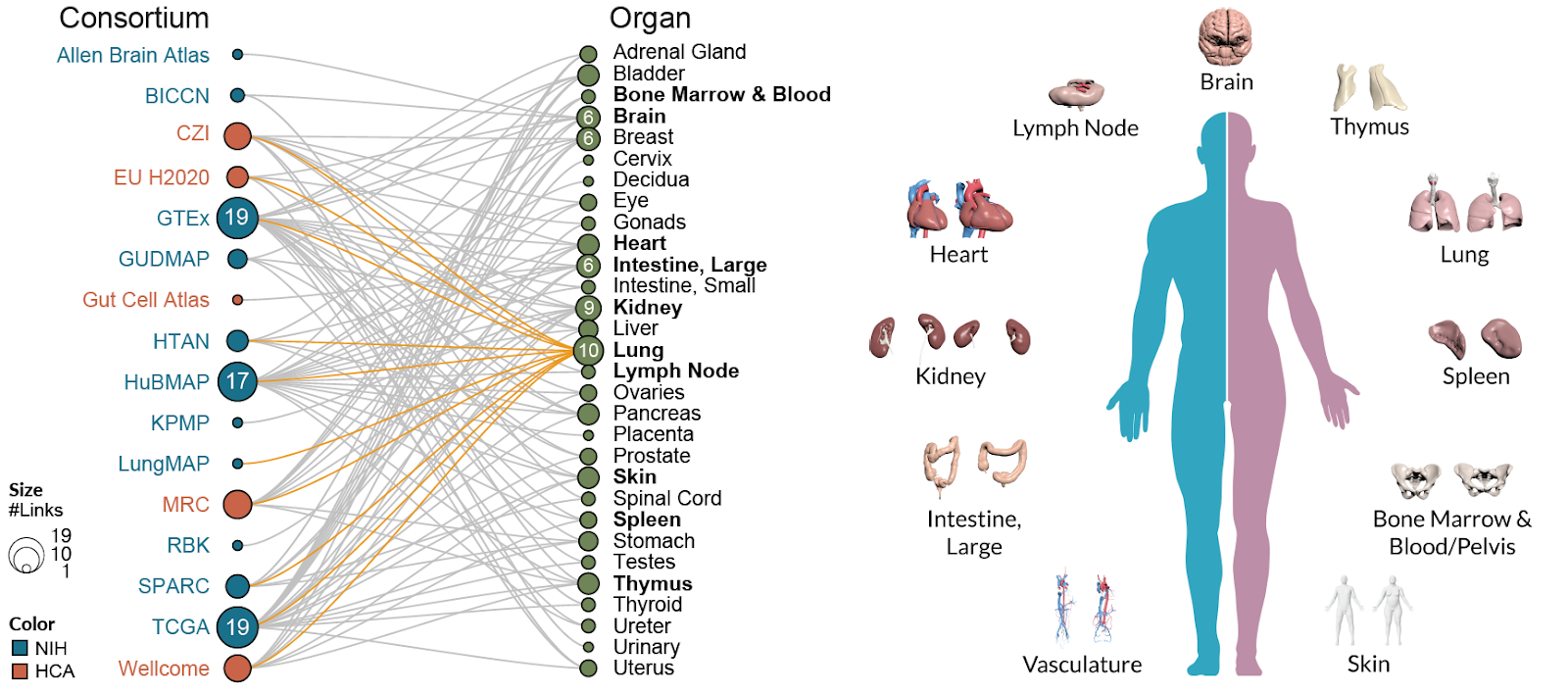
Astronomers mapping the observable universe find millions of galaxies. Biologists mapping the molecular and cellular universe of the human body is a galactic undertaking in its own right. The HuBMAP Consortium is working to chart the human body at the single-cell level (click here to enlarge the image above). “To create a 3D atlas of all these cells, tissues, and organs --I think some group is going to do it,” Thyagarajan said. “I foresee it first being done in experimental animals and then in humans. It will take time.”
Thyagarajan projects that the use of AI and digital pathology in differential diagnosis will be common in a decade. By then, spatial omics instrumentation will have reached a plateau and stabilized. The integration of the tools and techniques will take a little longer. In any event, the MPG spatial omics initiative is auspiciously timed. “We are on the bleeding edge.”
Illustration above the title: Deep infrared image of a galaxy cluster by NASA’s James Webb Space Telescope with a human-shaped silhouette superimposed. NASA.gov




{kind=link}