Program Details
Balance. Advocacy. Mentorship.
This four-year program prepares residents for practice in the setting of their choice. Our graduates thrive as fellows, chief residents, primary care providers, hospitalists, international and social medicine health experts, and faculty teaching the next generation of MedPeds providers.
Program Details
- Evaluation & Mentorship
- Continuity Clinics
- Schedules & Rotations
- Pathways
- Equity
- Stipends & Benefits
Resident Assessment and Coaching Committee (RAC)
We are committed to developing thoughtful, caring, and competent Internists-Pediatricians. We provide the feedback and coaching you need to become the best resident and career physicians that you can be. Each resident is assigned to a primary and secondary coach within the Resident Assessment and Coaching (RAC) Committee--a group of carefully-selected Med-Peds faculty who have close connections to the residency program and are known to be talented clinicians and supportive medical educators. It supports a holistic, timely, formative, and sustainable approach toward resident evaluation and development, focusing as much on identifying and developing strengths within each resident as on identifying opportunities for improvement. This committee also serves as our program's Clinical Competency Committee (CCC), an ACGME requirement* for all programs. RAC coaches follow residents throughout their residency, synthesize and interpret evaluations and other data, and help residents identify and achieve their own clinical and professional development goals. Coaches also serve as an additional resource for clinical questions and providing perspective, professional development, and connecting residents with other sources of mentorship.
Semi-Annual Reviews
Each resident meets with Dr. Aylward and an assigned APD--either Dr. Williams or Dr. Bhatt--twice a year to discuss and address topics pertinent to your development as a MedPeds resident. Semi-annual reviews help set clear expectations, reinforce the values of our profession, promote habits of competence, measure progress and provide objective feedback on resident performance, promote an individualized learning plan, and identify and address areas of concern. These meetings are meant to advance as the resident does, starting with interns transitioning into residency, continuing in the second year with becoming a senior resident, entering the third year with finding mentorship, scholarship and community partners, and finally into fourth year with job or fellowship guidance. These meetings also meet an ACGME requirement* on resident evaluation.
Twin Cities Med-Peds Alumni Network
The UMN Med-Peds Program additionally benefits from its vast network of alumni in the area who continue their clinical practice in a wide range of disciplines. Many alumni are primary care clinicians, Med-Peds hospitalists, some mix of the two, or sub-specialty trained and can offer current residents mentorship as they work towards their own professional aspirations.
Our Model
We value continuity clinics as much as inpatient and consult rotations. Our model maximizes residents’ time and continuity within clinics, minimizing transitions between inpatient obligations and clinic. We integrate longitudinal clinic-based quality improvement projects with team-based care initiatives.
How Continuity Clinics work
- Residents attend a full day of clinic each week while on outpatient, consult, and Children's Emergency Department rotations. This format supports continuity and acknowledges that patients typically seen in the morning differ demographically than those seen in the afternoon. It also allows for dedicated lunch hour teaching time.
- Residents have their own schedule when working in their continuity clinic.
- Residents do not attend clinic while on inpatient rotations, except for eight half-day clinic afternoons during pediatric inpatient rotations the intern year. This alleviates the stress of moving between inpatient and clinic-based responsibilities, improving teamwork and efficiency in both settings.
- Clinic staffing drives our templated resident schedule system. Residents are split into clinic- and day-specific teams. At any given time, half of the team will be on an inpatient service, and half the team will be on an outpatient service. The team on outpatient service provides coverage and follow-up on patient issues for the inpatient team. This hand-off allows for the smooth flow of patient care across rotations.
Continuity Clinic Sites
The UMN MedPeds residency serves three continuity clinic sites, each with its own unique patient population and surrounding community.
Community-University Health Care Center (CUHCC)
CUHCC is a federally qualified health center and a department within UMN's Academic Health Center. It offers medical, dental, mental health, advocacy, legal, and other services, serving 11,000 patients per year. Its mission is transforming care and education to advance health equity.
M Health Fairview-Eagan Clinic
M Health Fairview-Eagan is a state-of-the-art primary care clinic providing innovative, high-quality care to a diverse suburban population. Founded in the 1990s by a UMN-trained MedPeds physician, residents rotating at this suburban clinic work solely with MedPeds preceptors.
Center for International Health (CIH) and Midway Clinics
The CIH was established in 1980 in response to the influx of Southeast Asians to Minnesota after the Vietnam War. Since then, patients from more than 30 countries use CIH as their primary care site.
HealthPartners Midway Clinic
The HealthPartners Midway clinic serves an inner-city population in St Paul and is resourced by HealthPartners, an integrated, nonprofit health care provider and health insurance company based in Minnesota.
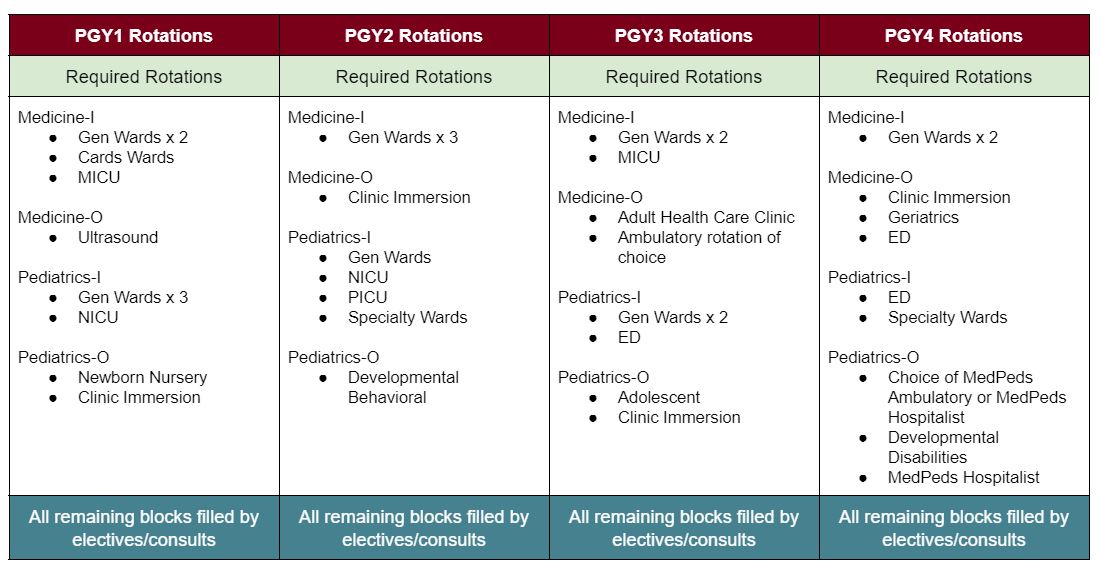
Schedules
Each MedPeds intern is assigned a four-year schedule template, indicating what type of rotation--Medicine Outpatient, Medicine Inpatient, Pediatrics Outpatient, Pediatrics Inpatient--they will be scheduled for at a given point in time. Templates are matched with continuity clinics, for the purpose of forming balanced clinic teams at each site. Rotation templates fulfill ACGME exposure requirements to each categorical specialty, as well as meet inpatient and consult/clinic requirements.
Sample schedule
Each residency year is split into 13 blocks. Each block is approximately 4 weeks in duration, although certain rotations occur in 2-week increments.
Rotations
Tailor your experience
Physician Advocacy Pathway
Clinician-Educator Pathway
Global Health
Hospital Medicine Pathway
Primary Care Pathway
Equity as a value and a practice
We value and build diversity within the physician workforce and promote a culture of belonging. Through leadership initiatives and feedback mechanisms, we work to flatten the hierarchy and put patients and residents at the center of all programmatic decisions:
- Ely RJ, Thomas DA. Cultural Diversity at Work: The Effects of Diversity Perspectives on Work Group Processes and Outcomes. Adm Sci Q. 2006;46(2):229. doi:10.2307/2667087
- Stahl GK, Maznevski ML, Voigt A, Jonsen K. Unraveling the effects of cultural diversity in teams: A meta-analysis of research on multicultural work groups. J Int Bus Stud. 2010;41(4):690-709. doi:10.1057/jibs.2009.85
- Association of American Medical Colleges (AAMC). Striving Toward Excellence: Faculty Diversity in Medical Education. Washington, DC; 2009. members.aamc.org/eweb/upload/Striving Towards Excellent Faculty Diversity in Med Ed.pdf. Accessed July 15, 2019.
- Cooper-patrick L, Gallo JJ, Gonzales JJ, Powe NR, Nelson C, Ford DE. Race, Gender, and Partnership in the Patient-Physician Relationship. J Am Med Assoc. 1999;282(6):583-589.
- Saha S, Komaromy M, Koepsell TD, Bindman AB. Patient-physician racial concordance and the perceived quality and use of health care. Arch Intern Med. 1999;159(9):997-1004. doi:10.1001/archinte.159.9.997
- Alsan M, Garrick O, Graziani GC. Does Diversity Matter For Health? Experimental Evidence from Oakland. Cambridge, MA; 2019. nber.org/papers/w24787.pdf.
- Smedley BD, Stith AY, Nelson AR. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Washington DC: The National Academies Press; 2003. doi:10.17226/10260
- Corporate Leavers Survey 2007: The Cost of Employee Turnover Due Solely to Unfairness in the Workplace. 2007. lpfi.org/sites/default/files/corporate-leavers-survey.pdf.
- Roberson QM, Colquitt JA, Roberson QM. Shared and Configural Justice : a Social Network Model of Justice in Teams. Acad Manag Rev. 2005;30(3):595-607.
- Cropanzano RS, Ambrose ML, Kulik CT, Li Y. The Fork in the Road: Diversity Management and Organizational Justice. Oxford Handb Justice Work. 2015;(June 2018). doi:10.1093/oxfordhb/9780199981410.013.27
- Milem JF, Chang MJ, Antonio AL. Making Diversity Work on Campus: A Research-Based Perspective. Washington, DC; 2005.
- Castillo-Page L. Assessing the Climate and Culture Around Diversity and Inclusion in Academic Medicine. Acad Med. 2012;87(10):1313.
- Milem JF, Dey EL, White CB. Diversity Considerations in Health Professions Education. In: Smedley B, Butler A, Bristow L, eds. In the Nation’s Compelling Interest: Ensuring Diversity in the Health-Care Workforce. Washington, DC: National Academies Press (US); 2004:345-390. ncbi.nlm.nih.gov/books/NBK216014/?report=reader.
Rates for 2025 - 2026 and 2026 - 2027
- PGY1: $71,862 annual, $2,753.32 biweekly
- PGY2: $74,073 annual, $2,838.05 biweekly
- PGY3: $76,589 annual, $2,934.43 biweekly
- PGY4: $79,415 annual, $3,042.71 biweekly
Educational Allowance
- $300 per residency year, for a total of $1200 throughout the course of residency
- Examples of eligible expenses include (but are not limited to) books, journal subscriptions, medical software, travel to scientific/medical conferences, board prep materials, cost of ABP board exam, cost of Step 3 exams, & medical licensure.
Insurance, Tax, Tuition Benefits
- Health insurance: single and family coverage
- Optional prescription, dental, vision insurance
- Life insurance: $50,000 basic group term life and AD&D insurance provided by the university. Supplemental plans are available.
- Disability insurance: residents are automatically enrolled in short and long-term disability insurance
- Malpractice insurance
Tax Benefits
- Health care flexible spending account
- Dependent day-care flexible spending account
- Optional retirement plan contributions, deferred compensation plan
Tuition
- In-state University of Minnesota tuition rates for spouse and immediate family
PTO & Leave Benefits
- 24 days per residency year, for total of 96 days throughout the course of residency
- 4 additional professional development/advocacy days.
- PTO is used for conference and fellowship interview travel, sick time, personal vacation, volunteer or advocacy work, and dedicated intern vacation time.
- PTO balances do not roll over from one residency year into the next.
- Paid parental leave
On-the-Job Benefits
- Access to departmental iPad, by request
- Free parking at all sites during rotations and clinics
- Discounted metro passes
- Embroidered lab coats, scrubs
- Lunches at core conferences
- Meal allowance on inpatient service
- Child care centers at UMN and VAMC
Additional Benefits
- Free access to campus libraries
- Free Google Suite access
- Free Medline searches, MD consults, and many other online databases and journals
- Discounts on a myriad of events and services: professional and collegiate athletics, fine arts, movies, technology, museums, film, state fair, home services, professional services, events coordination, and more
- Photocopying privileges
- Spouse/significant other group
- Access to the UMN Rec Center, and site-based fitness facilities
Certifications
All MedPeds residents are required to have certification in BLS, ACLS, PALS, and NRP prior to the start of rotations during intern year. Prior to the start of intern orientation, incoming interns must have valid BLS and ACLS certification. During intern orientation, the program will provide PALS and NRP. The residency can assist in arranging re-certifications for advancing senior residents.

