
J.E.D.I.
Department Statement on Antiracism
The Department of Family Medicine and Community Health mourns the unconscionable and senseless death of George Floyd on May 25, 2020. We believe that Black Lives Matter. We stand against racism in all its forms. We acknowledge that racism is a public health crisis.
Black, Indigenous, and people of color in Minnesota and elsewhere have been systematically marginalized and oppressed, and these communities have experienced over-policing, violence, structural and interpersonal racism, and disinvestment for years. Mr. George Floyd's horrific death during an arrest despite asking for help repeatedly and the related delay in formal charges in late May of 2020 resulted in an expression of anger, fear, and pain that erupted and changed Minneapolis and all of our lives. Two of our residency clinics were physically damaged, and in North Minneapolis, patients were temporarily left without their primary care home.
The pain, anger, and grief that we collectively and individually experienced must spur us to transformative action. This is a critical time in our society and we cannot be complacent and thus complicit in ongoing structural racism around us.
As a Department, we are intentionally, and imperfectly, working toward equity, inclusion, and justice. We will hold space for righteous anger and visionary passion while crafting a future that is honest about our contributions to oppression and racism and working with humility on a way forward.
We are committed to continuing the necessary and challenging work of antiracism in our clinical care, our educational programs, our eight residency programs and our rotations in the University of Minnesota Medical School, and our departmental structures and policies and environment that impact faculty and staff. We must recognize our complicity and identify the architecture of systemic racism and oppression that currently exists. As we enact new systems, many of the old systems must be repaired or completely dismantled, and we will not shy away from this essential work.
We encourage everyone, particularly those of us who are racialized as white, to educate themselves without placing the burden on colleagues/friends of color. As a Department, we will provide opportunities and resources to learn and grow individually and together, and we are cultivating an ecosystem of growth and learning that will allow courageous self-reflection and vulnerability to thrive. We will create a space for open dialogue and ongoing work in this field.
As a Department, we are going to live our values with opportunities to face this work head-on together. We have a responsibility to activate change and create a world that is safe and healthy for everyone.
- We view cultivating a growth mindset and a learning ecosystem, employing cultural humility and an understanding of power as essential components of creating an inclusive and integrated climate and culture that is safe, welcoming, respectful to all our learners, faculty, staff, and patients.
- Learn more about a growth mindset (coined by Carol Dweck): Growth Mindset - "Mindsets: A View from Two Eras," and "A Culture of Genius: How an Organization's Lay Theory Shapes People's Cognition, Affect, and Behavior"
Cultural humility is "a process that requires humility as individuals continually engage in self-reflection and self-critique as lifelong learners and reflective practitioners...that requires humility in how physicians bring into check the power imbalances that exist in the dynamics of physician-patient communication by using patient-focused interviewing and care, [and]...that requires humility to develop and maintain mutually respectful and dynamic partnerships with communities on behalf of individual patients and communities in the context of community-based clinical and advocacy training models." Read more about Melanie Tervalon and Jann Murray-Garcia's concept of cultural humility.
Power is a concept that is often not well-defined or understood but is incredibly impactful in leadership and relationships, including learner-educator and patient-provider relationships. Dr. Brené Brown lays out a valuable structure for thinking about power in her graphic.
Restorative justice (RJ) is an approach that embraces the reparation of harm and healing of trauma. A central practice of RJ is a collaborative decision-making process that necessarily includes harmed parties and can include people who have directly caused harm or simply others who are seeking active accountability. Accountability includes 1) accepting and acknowledging responsibility for causing harm, 2) repairing the harm caused to harmed parties and the community, 3) rebuilding trust by showing understanding of the harm, addressing personal issues, and building positive social connections, and 4) addressing root causes, systemic inequalities, and social injustices that create the conditions in which harm occurs (AAMC, Restorative Justice applications).
- Restorative Justice as the Rx for Mistreatment in Academic... : Academic Medicine
- Learn more about restorative justice in academic medicine on the AAMC website
- Anti-Racism Growth/Learning/Fear Zone graphic
- White Supremacy Culture - Dismantling Racism
- Tema Okun's website on divorcing white supremacy culture
- Brené Brown Unlocking Us Podcast on Shame
- Dr. Dafina-Lazarus Stewart - Language of Appeasement
- Continuum of Becoming an Antiracist Organization

(click to enlarge)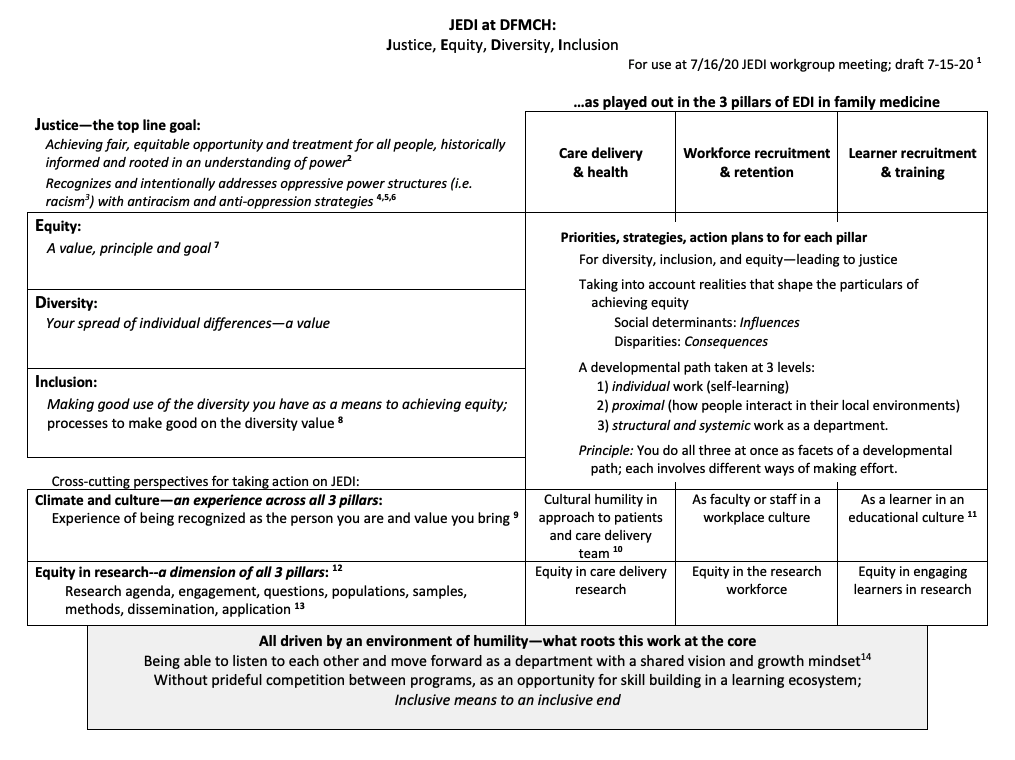
"The beauty of anti-racism is that you don't have to pretend to be free of racism to be an anti-racist. Anti-racism is the commitment to fight racism wherever you find it, including within yourself. And it's the only way forward." —Ijeoma Oluo
We believe in the DFMCH that this concept applies to all systemic oppressions, and we know we have work to do. In the paraphrased words of Brene Brown, we are committed to getting it right, not to being right.
Our developmental path includes simultaneous and integrated components:
- Individual work (self-learning)
- Proximal work (how people interact in their local environments)
- Structural and systemic work as a department
Why Justice?, an article by Andrea Westby, MD, vice chair for equity, diversity, and inclusion
Read our July 2020 issue of Family Medicine Monthly, a special edition devoted to racism and antiracism.
Bias Reporting at the University
Ethical Advocate and Bias Reporting and Response Network
Submit anonymous incident reports online at BRRN UReport or incident reports can also be sent to endbias@umn.edu.